
MSF has been treating many snakebite patients in its project in Agok in South Sudan. Until 2016, MSF was using an antivenom called FAV-Afrique to treat snakebite patients in Sub-Saharan Africa.
Two years down the line, we are now using two new antivenoms in South Sudan. While this is good news for our patients, this is not the solution for all snakebite victims. These antivenoms are specific to the snake species in this area and they are not largely available to those who need them.
For the nineteenth time, ten-year-old Awien is being taken into the operating theatre. Her right arm, damaged beyond repair, hangs limply in a sling around her neck. But at least she still has it. And most importantly, she is still alive.
Two months ago, Awien was bitten by a snake as she slept at night. Like many other snakebite victims across sub-Saharan Africa, reaching medical treatment in time was not a given for Awien. She lives in a small village in South Sudan, far from the nearest road and even further from the nearest hospital.
In rural areas like this, people’s first reaction to a snakebite is usually to treat it with traditional remedies. Awien’s family tried a number of things: a frog was cut in two and put on the bite to remove the venom; she was given a raw egg to drink and then a mixture of seeds and leaves to make her vomit so as to get the venom out of her body.
None of these remedies helped, so her uncle decided to carry her on his back to the nearest hospital. It took him a whole night to walk to Agok, where Doctors Without Borders (MSF) runs the only hospital in the region.
A big problem, little remedy

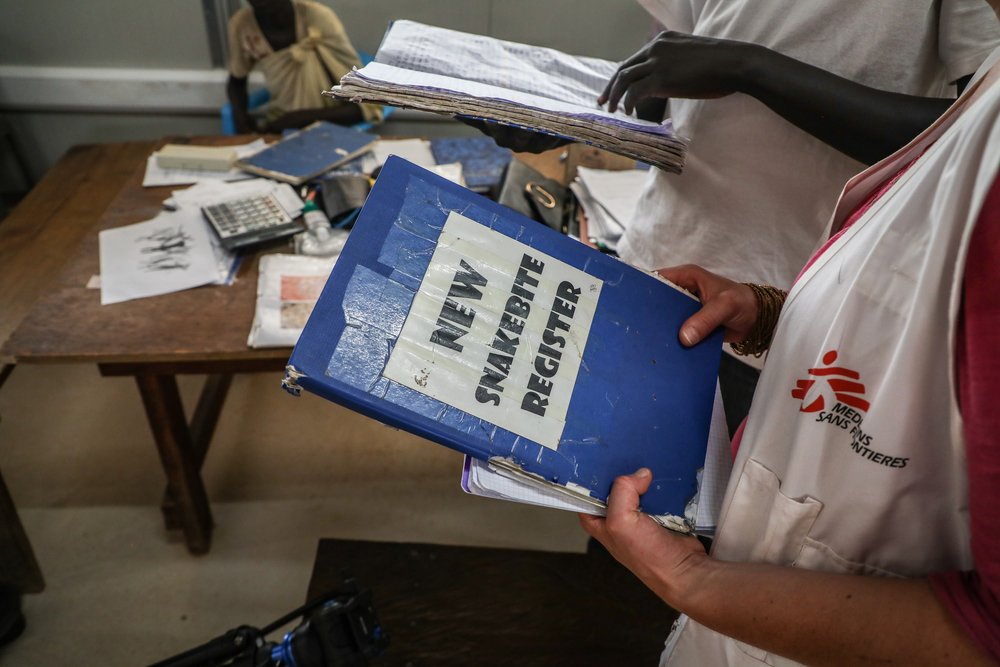
In Agok, MSF treats around 300 snakebite victims each year, most of them during the rainy season, which is when snakebites are most frequent. To escape the water, snakes often enter people’s houses, which is where about half of the victims are bitten.
Children playing outside and people working in the fields are also at risk. But wherever they are bitten, everyone has the same problem: how to get treatment. Most snakebite victims live in remote areas and have to travel long distances to seek care. During the rainy season, when roads can become impassable, people may have to travel for several days to reach a hospital.
In the village of Rumdong, a few hours by foot from Agok, the local leader, James Kuol War, tells how a man died this year after being bitten by a snake because he did not reach the hospital in time. Two other people in the same village, including a 13-year old girl, have been treated for snakebite at MSF’s hospital in the past year.
It is a longstanding problem. Another villager – a man in his seventies – says that he was lucky to survive two different snakebites in the same leg over the years. His foot is now badly misshapen, but he is otherwise healthy and can still fish and farm.
Globally, about 5 million people are bitten, and about 100,000 people die from snakebite every year, 30,000 of them in Africa. MSF clinical officer Jacob Chol Atem explains: “Some people come too late and some don’t come at all, so we don’t actually know the full extent of the snakebite burden in the area. But we do know it is a big problem and that people lose their lives because they can’t get treatment.”
Antidote out of reach and out of the price

MSF
Snakebite envenoming – the medical condition resulting from a snakebite – needs to be treated with antivenom in most cases. But antivenom is expensive and not available in many health facilities. It can cost several hundred rands per patient, more than a year’s salary for many people, especially those in rural areas, where most snakebite victims live.
Snakebite is a poor person’s disease, but pharmaceutical companies don’t create medicines for the poor; they create products that will be lucrative. Previously, MSF used an antivenom called FAV-Afrique, an all-in-one antivenom that was used to treat envenoming from ten different snake species in sub-Saharan Africa.
But the manufacturer decided to stop producing it and the last batch expired in June 2016. As there was no equivalent available, MSF had to find suitable alternative treatments. Two years down the line, MSF medical teams are now successfully using two new antivenoms in South Sudan: EchitabPlus and SAIMR-Polyvalent.

Atem says: “Before it was more straightforward: we could give the same antivenom even if we didn’t know which snake the patient had been bitten by. Now, the treatment has become more complex and we administer antivenom depending on the patient’s symptoms. But overall, it works and we are glad to have found an alternative.”
Whilst this is good news for MSF patients in Agok, this is not the solution for all snakebite victims, as choosing among 2 antivenoms based on symptoms is difficult for non-specialists. Antivenoms that are effective against venomous snakes in any given area need to be made available in all health facilities, but the high price of these antivenoms is a problem.
It is a vicious circle, where countries don’t buy antivenoms for their hospitals because they are too expensive, and pharmaceutical companies don’t make them because so few buyers are purchasing them. The result is that they remain largely out of reach of the people who need them.
Antivenom is not always enough

Even with antivenom, treatment for snakebite is much more difficult when victims arrive late at the hospital. Delays can cause further damage, including ‘compartment syndrome’, when swelling caused by the venom increases pressure within a muscle compartment, to the point that blood cannot supply the muscles and nerves with oxygen and nutrients.
If left untreated, muscles and nerves fail and may eventually die. Once acute compartment syndrome has occurred, surgery is the only option. In the most severe cases, the damage may be so extensive that patients lose the use of their limbs or need amputations. An estimated 400,000 people globally are maimed or disabled every year as a result of snakebite.
The long road to a cure
Awien has been at the hospital for two months now. She was in a critical condition when she arrived and was treated with three doses of antivenom. She was unconscious for the first five days, but eventually, she woke up and her condition started to improve.
She has had multiple surgeries to remove dead tissue, as the muscles in her arm were damaged beyond repair as a result of compartment syndrome. Nineteen surgical procedures sound like an awful lot, but her family did not want her arm amputated and asked the medical team to do all they could to save it. Awien was lucky to get treatment; this is not the case for countless others.
Find out more about MSF's work in South Sudan